General description
Tobacco, a plant with a long and complex history, has been utilized for centuries for its medicinal and recreational properties. Unfortunately, tobacco use has become a leading cause of preventable deaths worldwide. The Nicotiana genus includes sixty-seven species of annuals, biennials, perennials, and shrubs native to America and Australia. The commercial tobacco plant, used for producing tobacco products, was first used by Native Americans for medicinal and spiritual purposes. When Europeans arrived in the Americas, they discovered tobacco and cultivated it. By the 16th century, tobacco had become a commodity traded globally.
Tobacco cultivation is a labor-intensive process that requires significant management inputs. The cultivation process involves several steps: seeding, transplanting, weeding, and harvesting. After harvesting, the tobacco leaves are dried, cured, and fermented to develop their flavor and aroma. Tobacco cultivation has significant economic impacts, as it generally produces high returns on investment. However, the introduction of commercial tobacco production in areas where it was not previously grown has led to the displacement of other crops, resulting in a focus on a single cash crop.
The various species of Nicotiana are grown for different purposes. Earlier introduced species are produced for the fragrance of their warm-weather flowers, which typically open at night. However, newer strains of Nicotiana have flowers that remain open all day but have limited perfume. They are suitable for cutting, although the plants are sticky to handle. Nicotiana tabacum, the most commonly used species of tobacco, is a member of the Solanaceae family. Historically, Nicotiana tabacum was known for its medicinal properties, and nicotine was successfully identified from tobacco leaves.
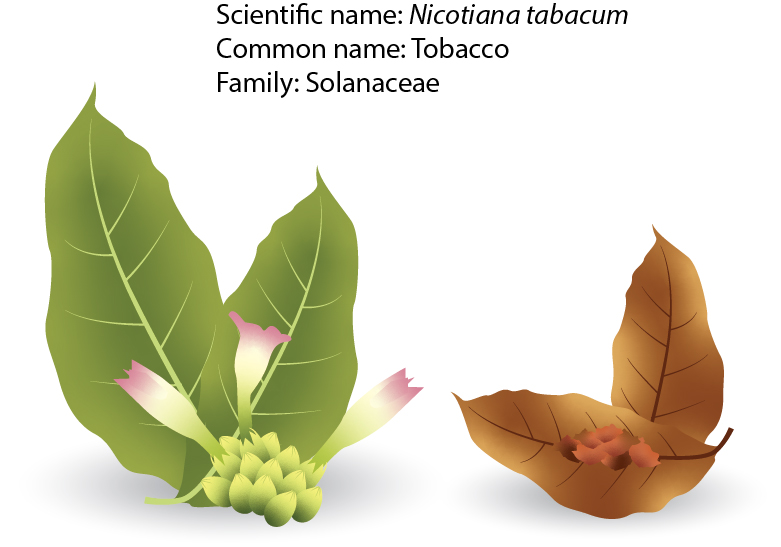
Tobacco is primarily grown in warm climates with moderate rainfall, and it is widely cultivated worldwide in tropical and subtropical regions, including North and South America, Europe, Africa, and Asia. The plants can spread quickly in large areas such as forests, mountains, dry valleys, wetlands, and savannahs. Nicotiana tabacum and Nicotiana rustica are the two preferred species for the economic crop. The most commercial part of the plant is the leaf, and the best time for harvesting the leaves is during a dry period. The leaves are green, oval-shaped, and can reach a length of fifty centimeters. The height of N. tabacum is typically 1.5 to 2 meters. This plant has branching stems and short flowers with white, pink, or reddish-colored limbs.
Nicotiana tabacum is a robust annual herb that grows to heights between one to two meters and has large green leaves that are oblong-lanceolate and acuminate. The lower semiamplexicaul and decurrent leaves are long and trumpet-shaped, with white-pinkish, rosy, or reddish flowers that are pedicelled and four to five centimeters long. These flowers are found in many-flowered, usually panicled racemes. The capsule of Nicotiana tabacum is 1.5-1.8 cm long, a little longer than the calyx. All parts of the herb are sticky and covered with short viscid glandular hairs, which exude a yellow secretion that contains an alkaloid known as nicotine.
Tobacco cultivation has a rich history and was first cultivated in pre-Columbian times in the West Indies, Mexico, and Central America. Today, it is cultivated worldwide, with the tobacco plant thriving best in soil rich in vegetable mould. Although it is marginally frost hardy to frost tender, the tobacco plant needs full sun or light shade and fertile, moist, but well-drained soil. The plant is propagated from seed in early spring, and the seed of certain varieties requires a weak stimulus for germination. It is unnecessary to supply the necessary plant food to keep the soil in good physical condition.
Tobacco leaves are picked as they mature or are harvested together with the stalk. The tobacco leaves are cured, fermented, and aged to develop an aroma and reduce the harsh, rank odor and taste of fresh leaves. However, tobacco was not only sniffed and smoked but chewed, eaten, drunk (like tea), smeared over bodies (to kill lice and other parasites), and used in eye drops and enemas.
Tobacco use is the leading preventable cause of premature death worldwide, and it is estimated that 4.9 million people died of tobacco-related illness in the year 2000. Unfortunately, this figure is projected to rise to ten million deaths annually by the 2020s, with seventy percent of those deaths occurring in developing countries. In addition, tobacco use is a significant independent risk factor for developing oral and pharyngeal cancer, as well as other malignancies of the upper aerodigestive tract.
Tobacco is consumed in various ways, with manufactured cigarettes being the most prevalent form of use. Although smokers know tobacco is harmful to health, they often underestimate its risks. Furthermore, the public is generally unaware of the full spectrum of health risks associated with tobacco use. For example, in the UK, only 2/3rd of the general public is aware that smoking may cause oral cancer, suggesting that smokers are likely underestimating their risk.
For many tobacco users, the situation is complicated by solid nicotine dependence and multiple barriers to cessation. However, it is essential to note that tobacco (nicotine) dependence treatment has the potential to save many millions of lives. Therefore, it is critical to promote awareness of the dangers of tobacco use and increase access to cessation programs for those who are struggling with addiction.
Medical and pharmacological usage
Tobacco contains more than 7,000 chemicals, including nicotine, tar, carbon monoxide, and various carcinogens. Nicotine, a highly addictive stimulant, is responsible for the pleasurable effects of tobacco use. Tar, a sticky substance formed when tobacco is burned, contains carcinogens that can cause cancer. Carbon monoxide, a toxic gas, reduces the amount of oxygen in the blood, leading to various health problems.
While the whole plant, including leaves, flowers, seeds, roots, and individual chemical constituents, have been used traditionally and medicinally, tobacco is also commonly abused worldwide as a local irritant. When used as snuff, it causes violent sneezing and copious mucous secretion. Chewed, it irritates the mucous membrane of the mouth, increasing the flow of saliva. Injected into the rectum, it acts as a cathartic.
Tobacco use is a leading cause of preventable deaths worldwide, responsible for several health problems, including cancer, cardiovascular disease, respiratory disease, and reproductive disorders. Large doses of tobacco can cause nausea, vomiting, sweats, and great muscular weakness. Nicotine, the alkaloid present in tobacco, is a virulent poison that can produce significant digestive and circulatory disturbances, heart palpitations, cardiac illness, and vascular contraction and is considered one of the causes of arterial degeneration.
The effects of nicotine depending on the rate and route of delivery and the development of tolerance. While there has been more research on smoked tobacco than on oral use (smokeless) tobacco, both methods result in systemic absorption of pharmacologically significant amounts of nicotine. Although absorption of nicotine through the buccal mucosa is slower than through the pulmonary route and leads to lower arterial levels, regular users of each product have similar venous nicotine levels.
Nicotine is a highly alkaline volatile oil with an acrid smell and burning taste. It is one of more than seven thousand chemicals in tobacco, along with tar, carbon monoxide, and various carcinogens. Nicotine is responsible for the pleasurable effects of tobacco use and is highly addictive. When tobacco is burned, tar is formed, which contains several carcinogens, and carbon monoxide is released, reducing the amount of oxygen in the blood and leading to various health problems.
Tobacco was once used as a relaxant, but it is no longer employed except occasionally in chronic asthma. Although it has some medicinal uses, it can be toxic and even fatal if applied topically in excess. The smoke from tobacco acts on the brain, causing nausea, vomiting, and drowsiness. It is sometimes used as a sedative, diuretic, expectorant, discutient, and sialagogue, and in rare cases, as an emetic. In the past, nicotine salicylate was used to treat scabies, and nicotine was also used for patients with Parkinson’s disease. However, only a limited number of studies have been conducted on the therapeutic effects of N. tabacum and its chemical constituents and pharmacological effects.
Secondary metabolites are chemical constituents with carbon skeleton structures called compounds with some biological activity effects. N. tabacum is rich in secondary metabolites, including phenolics, terpenoids, and alkaloids. The tobacco leaf contains several pyridine alkaloids, with nicotine being the most significant. Other alkaloids present include nicotimine, anabasine, anatalline, and nor-nicotine. It also has a high percentage of organic acids. Leaves also contain glucosides, tahacinin, tahacilin, and iso-quercitrin, as well as 1-quinic, chlorogenic, caffeic, and oxalic acids. Tobacco leaves also contain terpenic and carcinogenic substances.
Anatabine and (+)nornicotine have been isolated from the roots of the tobacco plant. Quercetin-3,3-dimethyl ether and quercetin-3-Me ether are flavonoids isolated from tobacco flowers. Three new gibberellins, named nicotiana α, β and γ, have been identified, along with gibberellins A and A3, in shoot apices and flower buds of the tobacco plant. The seed of the tobacco plant contains various compounds, including cycloartanol, cycloartenol, 24-daturadiol and solavetivone. The seed oil also has a variety of compounds, such as cholesterol, cholest-7-enol, campesterol, stigmasterol, sitosterol, and lanosterol. Other compounds in the seed oil include 28-isofucosterol, 31-norlanosterol, lanost-8-enol, obtusifoliol, 31-norcycloartenol, cycloeucalenol, granisterol, citrostadienol, β-amyrin, lupeol, cycloartanol and 24-methylenecycloartanol. Anatabine and (+)nornicotine have been found to have potential anti-inflammatory and neuroprotective effects, while quercetin is a flavonoid with antioxidant and anti-inflammatory properties. Gibberellins are plant hormones that regulate growth and development, including stem elongation and flower formation. The compounds found in tobacco seed oil have potential health benefits, such as reducing cholesterol levels and anti-inflammatory effects.
The harmful effects of smoking tobacco have been extensively studied, and it is now known that after tobacco leaves are smoked, nicotine decomposes into a range of toxic substances, including pyridine, furfurol, collidine, hydrocyanic acid, and carbon monoxide. These toxic compounds are responsible for the poisonous effects of tobacco smoke. However, beneficial compounds can also be extracted from tobacco leaves. The white-brown complex subfamily protein is one such compound. This odorless, tasteless powder can be extracted from tobacco leaves and added to various foods, including cereal grains, vegetables, and soft drinks. It can be whipped like egg whites, liquefied or gelled and can take on the flavor and texture of a range of foods. While the safety and potential health benefits of this compound are still being studied, it has the potential to be a valuable ingredient in the food industry.
Cigarette and cigar smoking
Cigarette smoke contains over seven thousand compounds and many harmful chemicals, such as nicotine, carbon monoxide, tar, benzene, and heavy metals. The incidence of non-communicable diseases has increased rapidly in many developing countries due to demographic and lifestyle changes. In low and middle-income countries, nearly half the disease burden is from non-communicable diseases, and more than twenty-one percent of deaths are due to cardiovascular diseases. Tobacco use is a significant risk factor for cardiovascular disease, including heart attacks and strokes. The chemicals in tobacco smoke can damage blood vessels and increase the risk of blood clots, leading to various cardiovascular problems. Globally, many risk factors for heart disease, diabetes, cancer, and pulmonary diseases are due to lifestyle and can be prevented. Tobacco use is the most significant among the risk factors for non-communicable diseases. It is a well-established cause of cancer and is also responsible for cardiovascular and chronic respiratory diseases. Smoking is a significant risk factor for respiratory disease, including chronic bronchitis and emphysema. The chemicals in tobacco smoke can damage the airways and reduce lung function, leading to various respiratory problems.
There are over 1.3 billion smokers worldwide, with approximately eighty-two percent residing in low and middle-income countries. Tobacco consumption and excessive alcohol use are major risk factors for cancers of the oral cavity and pharynx. The risk from these two agents is synergistic, and heavy smokers (40+ cigarettes/day) and heavy drinkers (30+ drinks per week) have a significantly higher risk of developing oral cancer than those who abstain from both products. The growth in smoking rates is typically followed by an increased incidence of diseases such as ischemic heart disease, lung, oral cavity, and larynx cancers ten to twenty years later.
The habit of reverse smoking, holding the burning end of cigarettes or cigars within the oral cavity, is strongly associated with palatal lesions and has a high risk of developing oral cancer. This habit is prevalent in India, South America, and the Philippines. Smoking bidis, hand-rolled tobacco wrapped in a tendu leaf, is a known risk factor for oral and pharyngeal cancer. The worldwide oral use of smokeless tobacco takes many forms, and the risks appear to differ depending on the processing of the product, which can markedly affect nitrosamine content.
Tobacco smoke comprises many carcinogenic compounds, with polynuclear aromatic hydrocarbons (PAHs) being the most predominant. PAHs are primarily contact carcinogens, and the principal PAH carcinogen in most target tissues is benzo-(a)pyrene, which is activated by P450 isoenzymes to the carcinogen metabolite benzo(a)pyrenedihydrodihydroxy epoxide. These metabolites react with DNA to form predominantly guanosine adducts, which can initiate carcinogenesis if not detoxified by glutathione S-transferases (GSTs). Chewing tobacco leads to local exposure of the oral mucosa to tobacco-specific nitrosamines, and Sudanese oral snuff (toombak) and Indian tobacco chewers have been found to have unusually high levels of carcinogenic tobacco-specific nitrosamines in their saliva.
Smoking not only affects the smoker but also exerts indirect adverse effects on the fetus by altering umbilical blood flow and direct impact through the placental transfer of toxins. Due to its high lipid solubility, nicotine and its primary metabolite, cotinine, readily cross the placental tissue into the fetal bloodstream. The fetus is found to have greater exposure to nicotine than the smoking mother, as measured by nicotine levels in amniotic fluid and fetal plasma. Epidemiological studies have shown a dose-related effect of smoking on conception, with a delay of about two months. Tobacco use is a significant risk factor for reproductive disorders, including infertility, miscarriage, and low birth weight. The chemicals in tobacco smoke can damage the reproductive organs and reduce fertility, leading to various reproductive problems. Studies have shown that smoking is associated with a delay in conception and infertility, and recent research indicates that prenatal smoking is linked to overweight and obesity in offspring later in life.
Secondhand smoke, also known as passive smoking, is the smoke that is exhaled by a smoker or comes from the burning end of a cigarette, cigar, or pipe. It contains the same harmful chemicals as mainstream smoke and can cause various health problems, including cancer, cardiovascular disease, and respiratory disease. Non-smokers exposed to secondhand smoke have an increased risk of developing lung cancer, heart disease, and stroke, among other health problems.
Tobacco dependence
Over the past two decades, there has been significant research into the pharmacological effects of nicotine and the pathophysiology of nicotine addiction. Nicotine, like other addictive drugs, affects mood and performance and exhibits all the classic hallmarks of drug addiction. The primary criteria for classifying addictive drugs are compulsive use, psychoactive effects, and drug-reinforced behavior. Other measures include stereotypic patterns of use, use despite harmful consequences, relapse following abstinence, and cravings or urges to use. Dependence-producing drugs also often produce tolerance, physical dependence (withdrawal symptoms), and pleasant subjective effects. Whether smoked or used in a smokeless form, tobacco meets all of these criteria.
After each cigarette, blood nicotine levels decrease rapidly, while levels remain stable during and after smokeless tobacco use. With smokeless tobacco, nicotine absorption continues even after the tobacco is discarded from the mouth due to the release of nicotine from the mucous membranes and the absorption of swallowed nicotine. The systemic absorption of nicotine per typical dose maybe three to four times greater for smokeless tobacco than for smoked tobacco. The short half-life of nicotine (2 hours) accumulates throughout the day in regular smokeless tobacco users and persists overnight, leading to physical and psychological dependency.
Nicotine has several actions that can lead to dependence. Due to its action on pre- and post-synaptic neuronal nicotinic acetylcholine receptors, nicotine facilitates the release of several neurotransmitters, including acetylcholine, dopamine, noradrenaline, serotonin, beta-endorphin, and glutamate. Nicotine also stimulates the release of growth hormones, adrenocorticotropic hormones, and prolactin. However, the rewarding properties of nicotine are believed to be mediated by dopamine release in the nucleus accumbens, as is the case with other psychostimulant abuse drugs, which reinforces its self-administration.
Depending on the situation and baseline state of the individual, nicotine can have both positive and negative subjective effects. It can produce a sense of well-being, reduce anxiety, help maintain cognitive vigilance, and have both arousing and relaxing effects. However, it is not clear to what extent these positive subjective effects reported by tobacco users are the result of the primary intrinsic impacts of nicotine and to what time they reflect relief of withdrawal symptoms which can appear after only a couple of hours of abstinence. Nicotine also causes functional and structural changes in the central nervous system, including upregulation of the density of nicotinic receptors.
While approximately 90-95% of people who use tobacco do so every day and show varying degrees of nicotine dependence, there exists a small minority who use the drug on an occasional basis (‘‘chippers’’) and, despite taking in a similar amount of nicotine per cigarette as regular daily smokers, show no signs of dependence. Cigarettes, on average, contain about 12 milligrams of nicotine, of which the smoker typically absorbs about one to two milligrams. Nicotine withdrawal symptoms, believed to be the reason tobacco users relapse in the short term, have been studied more thoroughly in smokers than in smokeless tobacco users. They include irritability, impatience, restlessness, difficulty concentrating, difficulty sleeping, increased appetite, particularly for sweet and high-carbohydrate foods, weight gain, anxiety, and depressed mood.
The predominantly affective withdrawal symptoms begin in a minor form a few hours after the last cigarette, as nicotine blood levels drop, and symptoms usually peak two to three days after quitting. If tobacco abstinence is maintained, mood usually returns to baseline (pre-quitting) level after about three to six weeks, although there is much individual variation. However, the craving or urge to smoke cigarettes, increased appetite, and weight gain can continue for many months after quitting. Although data are much more limited on the acute withdrawal effects from smokeless tobacco, the symptoms appear to be very similar, though they may be less intense and fewer.
Tobacco dependence treatment
In developed countries, it is estimated that around 30 to 40 percent of smokers try to quit smoking every year. Unfortunately, without adequate support and assistance, only about 2 to 3 percent of smokers succeed in their attempt to abstain from smoking for at least a year. The realization of the persistent nature of nicotine addiction and the difficulty that most tobacco users face in overcoming it, even if they intend to quit, has prompted some countries to fund formal cessation programs, particularly in the United Kingdom.
The essential components of tobacco dependence treatment include assessing and, if necessary, enhancing the motivation to quit, evaluating the degree of nicotine dependence, providing counseling or behavioral support, and promoting appropriate pharmacotherapies (such as nicotine replacement therapy or bupropion) to alleviate the severity of withdrawal symptoms.
In the early 1900s, most tobacco use involved chewing tobacco, pipes, cigars, and snuff rather than cigarettes. However, the consumption of cigarettes has significantly increased since then and has become the primary mode of tobacco use in many countries, leading to a surge in tobacco-related health issues.
Despite the availability of various cessation aids, such as nicotine replacement therapy, bupropion, and varenicline, quitting smoking remains a challenging process for many smokers. Nevertheless, studies have shown that smokers who receive intensive behavioral support and pharmacotherapy are more likely to quit successfully than those who attempt to quit without assistance.
Moreover, it is worth mentioning that cessation efforts must continue even after a person has quit smoking, as relapse is common, particularly during the first few months after quitting. Therefore, follow-up care, counseling, and support are essential components of tobacco dependence treatment.
Methods to reduce demand
Tobacco control measures aim to reduce tobacco use and its health effects. These measures include tobacco taxes, smoke-free laws, health warnings, and tobacco cessation programs. Tobacco taxes, which increase the cost of tobacco products, have been shown to reduce tobacco use and generate revenue for the government effectively. Smoke-free laws, which prohibit smoking in public places, protect non-smokers from secondhand smoke and effectively reduce exposure. Health warnings and restrictions on advertising and promotion can increase awareness of the health risks of tobacco use and reduce the appeal of tobacco products.
Health warnings on tobacco products are an effective tobacco control measure, as they increase awareness of the health harms of tobacco use and encourage smokers to quit. Alternative tobacco products, such as e-cigarettes, smokeless, and heated tobacco products, have gained popularity as cigarette substitutes. While some of these products may be less harmful than cigarettes, they are not entirely safe and can still cause health problems. For example, e-cigarettes can still contain nicotine and other toxic chemicals, and their long-term health effects are unknown.
Education and persuasion have likely played a significant role in decreasing smoking prevalence in some Western countries. Increasing access to effective treatments to aid smoking cessation is another approach that has gained popularity. Many countries now restrict or ban the promotion of tobacco products and do not permit the sale of tobacco products to minors.
Raising the cost of tobacco use has proved to be an effective tobacco control strategy. Comprehensive bans on smoking in workplaces and indoor public areas also appear to have had an effect. The primary reason for introducing such bans is to protect the health and comfort of non-smokers, but bans can also motivate smokers to quit and make it easier for them to succeed.
While inhaling tobacco smoke will always be very harmful, there are ways to engineer cigarettes to reduce harm to human smokers. For example, using tobacco that is missing some of the known carcinogens or reducing the tar-to-nicotine ratio can help. However, the tobacco industry has a long history of opposing tobacco regulation and using various tactics to influence policy, such as funding research, lobbying governments, and advertising and marketing to promote their products. Governments must remain vigilant and enact effective measures to combat the harm caused by tobacco use.
Future of tobacco control
The Framework Convention on Tobacco Control is a global response to the threat posed by tobacco. It is the first-ever international health treaty and represents a significant achievement that, if ratified and implemented, would undoubtedly prevent the suffering and premature death of millions over the coming decades. 168 countries have signed the treaty, and 137 have ratified it. Notably, the United States and Haiti are among the countries that have signed but not ratified the treaty.
One way to jumpstart the ratification process is for every country to impose a levy on tobacco products or tobacco industry profits, specifically for funding tobacco control. A levy on tobacco products would lead to an immediate reduction in smoking prevalence, and the funds generated could be directed to tobacco control task forces in each country. Governments should legislate to ensure these funds are protected and cannot be diverted for other purposes. Concerns that such price increases could disadvantage the poor have been overstated and must be weighed against the significant health gains resulting from such measures. The levy could also fund treatment programs to aid smoking cessation.
Moving forward, much stricter regulation of toxin exposure from tobacco products should be a central plank of future tobacco control. Existing and proposed regulations on smoke constituents from manufactured cigarettes are unlikely to make a significant difference because they continue to allow high levels of exposure to human smokers. Therefore, governments should consider informing tobacco companies that beyond a designated timescale, their products will not be allowed to deliver more than trace amounts of known carcinogens or other toxins. Such regulations could see the end of smoked tobacco as the dominant means of ingesting nicotine. This can be achieved with smokeless products and would mark a significant step forward in global tobacco control.
In conclusion, while significant progress has been made in tobacco control, more needs to be done. The Framework Convention on Tobacco Control provides a solid foundation, but more concrete action is required, including levies on tobacco products, strict regulation of toxin exposure, and continued support for smoking cessation programs. Governments must work together to implement these measures and ensure they effectively reduce tobacco use and its harmful effects. By doing so, we can prevent the suffering and premature death of millions of people worldwide.
The use of tobacco in fundamental study
Tobacco has been widely used in fundamental scientific research for decades, due to its unique characteristics and properties. The plant has a relatively simple genome, and it is easy to grow and maintain in laboratory conditions. In addition, it can be manipulated genetically, allowing researchers to study the functions of specific genes and proteins.
One of the main ways tobacco has been used in fundamental research is as a model organism for studying plant biology. Tobacco plants are commonly used to investigate plant development, physiology, biochemistry, and genetics. Because of its relatively simple genome, tobacco is often used as a surrogate for other plant species that are more difficult to work with or that have more complex genomes. For example, tobacco has been used to investigate the mechanisms of photosynthesis and the pathways of carbon metabolism.
Tobacco is also widely used in molecular biology research. It is an important host for the production of recombinant proteins and is commonly used as a model organism for the study of protein-protein interactions, gene regulation, and signal transduction. Tobacco is used in the production of biopharmaceuticals, vaccines, and diagnostic reagents, due to its ability to produce large quantities of recombinant proteins.
In addition to being used as a model organism for plant and molecular biology research, tobacco has been used in several other fundamental scientific studies. For example, it has been used to investigate the mechanisms of plant-pathogen interactions, including the molecular and biochemical events that occur during plant defense responses. Tobacco has also been used in studies of plant stress responses, such as the effects of drought, salinity, and temperature stress on plant growth and development.
Tobacco has also been used in environmental research, particularly in studies of air pollution. Tobacco plants are sensitive to air pollutants such as ozone, nitrogen oxides, and sulfur dioxide, and have been used to study the effects of these pollutants on plant growth and development. The use of tobacco in such studies has contributed to our understanding of the impacts of air pollution on ecosystems and human health.
Another area of fundamental research where tobacco has been used is in studies of human health. Tobacco contains numerous toxic and carcinogenic compounds, and its use has been linked to a range of health problems, including lung cancer, cardiovascular disease, and respiratory illness. Tobacco has been used as a model organism for the study of these diseases, allowing researchers to investigate the mechanisms by which tobacco use contributes to their development.
In conclusion, tobacco has been an important tool in fundamental scientific research for decades. Its unique properties and characteristics have made it an ideal model organism for studying plant and molecular biology, as well as environmental and human health. The use of tobacco in these studies has contributed significantly to our understanding of a wide range of scientific fields and has helped to improve human health and well-being.
Here are some of the other species of Nicotiana mentioned in the statement and their uses:
Nicotiana alata syn. Nicotiana affini is commonly known as jasmine tobacco due to its sweet, floral fragrance. It is often grown as an ornamental plant in gardens and is also used in producing perfumes. Nicotiana bigelovii syn. Nicotiana quadrivalvis is also known as Indian tobacco or sacred tobacco. Indigenous people in North America have used it for centuries for medicinal and ceremonial purposes.
Nicotiana glauca is commonly known as tree tobacco or mustard tree. It is a large shrub or small tree native to South America but has been introduced to other parts of the world. The leaves and sap of the plant contain nicotine, which is sometimes used as a natural insecticide. Nicotiana langsdorfii is often called Langsdorff’s tobacco. It is an annual plant that produces small, yellow flowers and is often grown as an ornamental plant in gardens. Nicotiana rustica is also known as wild tobacco or Indian tobacco. It is native to South America and is often used for ceremonial and medicinal purposes. It contains a high nicotine level and is more potent than Nicotiana tabacum. Nicotiana x sanderae is a hybrid of Nicotiana forgetiana and Nicotiana paniculata. It is often grown as an ornamental plant and produces colorful flowers.
Nicotiana sylvestris is commonly known as woodland tobacco. It is an annual plant that produces white, trumpet-shaped flowers and is often grown as an ornamental plant in gardens. Overall, while Nicotiana tabacum is the most commonly known species of Nicotiana due to its use in tobacco products, other species of the plant have various benefits, including ornamental plants and their psychoactive effects.
Further readings:
Al-Snafi, A. E. (2022). Pharmacological and toxicological effects of Nicotiana tabacum. World, 3(01), 006-018.
Anderson, P. (2006). Global use of alcohol, drugs and tobacco. Drug and alcohol review, 25(6), 489-502.
Arcury, T. A., & Quandt, S. A. (2006). Health and social impacts of tobacco production. Journal of agromedicine, 11(3-4), 71-81.
Billings, E. R. (2019). Tobacco; its history, varieties, culture, manufacture and commerce. Good Press.
Carmody, T. P. (1989). Affect regulation, tobacco addiction, and smoking cessation. Journal of psychoactive drugs, 21(3), 331-342.
Guindon, G. E., & Boisclair, D. (2003). Past, current and future trends in tobacco use.
Istvan, J., & Matarazzo, J. D. (1984). Tobacco, alcohol, and caffeine use: a review of their interrelationships. Psychological bulletin, 95(2), 301.
Lemyre, A., Poliakova, N., & Bélanger, R. E. (2019). The relationship between tobacco and cannabis use: a review. Substance Use & Misuse, 54(1), 130-145.
Lock, C. G. W. (Ed.). (1886). Tobacco: Growing, Curing, & Manufacturing: A Handbook for Planters in All Parts of the World. E. & FN Spon.
Morissette, S. B., Tull, M. T., Gulliver, S. B., Kamholz, B. W., & Zimering, R. T. (2007). Anxiety, anxiety disorders, tobacco use, and nicotine: a critical review of interrelationships. Psychological bulletin, 133(2), 245.
Murin, S., Rafii, R., & Bilello, K. (2011). Smoking and smoking cessation in pregnancy. Clinics in chest medicine, 32(1), 75-91.
Putri, D. A., Solihah, R., Oktavia, R., Anggraini, D. A., & Fatmawati, S. (2022). Secondary Metabolites of Nicotiana tabacum and Their Biological Activities: A Review. The Journal of Pure and Applied Chemistry Research, 11(2), 149-165.
Riquinho, D. L., & Hennington, E. A. (2012). Health, environment and working conditions in tobacco cultivation: a review of the literature. Ciência & Saúde Coletiva, 17(6), 1587-1600.
Sanjeev, A., & Kapgate, S. M. Tobacco (Nicotiana tabacum)-A Systemic Review. population, 51, 7.
Stedman, R. L. (1968). Chemical composition of tobacco and tobacco smoke. Chemical reviews, 68(2), 153-207.
Thun, M. J., Henley, S. J., & Calle, E. E. (2002). Tobacco use and cancer: an epidemiologic perspective for geneticists. Oncogene, 21(48), 7307-7325.
Tso, T. C. (1972). Physiology and biochemistry of tobacco plants. Stroudsburg, Pa., USA, Dowden, Hutchinson & Ross, Inc..
Vine, M. F. (1996). Smoking and male reproduction: a review. International journal of andrology, 19(6), 323-337.
Warnakulasuriya, S., Sutherland, G., & Scully, C. (2005). Tobacco, oral cancer, and treatment of dependence. Oral oncology, 41(3), 244-260.
West, R. (2006). Tobacco control: present and future. British medical bulletin, 77(1), 123-136.
West, R. (2017). Tobacco smoking: Health impact, prevalence, correlates and interventions. Psychology & health, 32(8), 1018-1036.
World Health Organization. (2017). Tobacco and its environmental impact: an overview. World Health Organization.